Femoral Acetabular Impingement
By Deborah Pate, DC, DACBR
Femoral acetabular impingement (FAI) is a major cause of early osteoarthritis or degenerative joint disease of the hip, especially in young, active patients. It is characterized by abnormal contact of the acetabulum and the femur during the limits of physiologic hip range of motion, particularly during flexion and internal rotation. Clinical manifestations of the syndrome include groin and/or posterior hip pain.1
FAI is classified as either "pincer" or "cam" impingement. The cam form comes from the Dutch word for cog; the femoral head has lost its spherical shape, which allows abnormal contact between the head of the femur and the acetabulum. The pincer form comes from the French word meaning to pinch; the acetabulum covers too much of the femoral head. This overcoverage results in the labral cartilage being pinched between the rim of the acetabulum and the anterior femoral head-neck junction.
Commonly, a combination of both forms exists, described as mixed. It is postulated that FAI may very well be a contributing pathway to the development of premature degenerative joint disease.2 The suspected etiology of this disorder is abnormal development of the physis, but it can also occur in slipped capital femoral epiphysis (SCFE), Legg-Calve-Perthes disease, and malunited femoral neck fractures.
 Lesions identified by imaging include characteristic tears of the anterior and posterior labrum, paralabral cyst formations and synovial herniation pits at the site of mechanical impact of the femoral neck, and osteochondral injuries of the acetabular roof and femoral head. However, the hip studies are often read as normal, particularly plain films. Many of the early findings are very subtle and frequently are considered normal.
Lesions identified by imaging include characteristic tears of the anterior and posterior labrum, paralabral cyst formations and synovial herniation pits at the site of mechanical impact of the femoral neck, and osteochondral injuries of the acetabular roof and femoral head. However, the hip studies are often read as normal, particularly plain films. Many of the early findings are very subtle and frequently are considered normal.
The first step in the assessment of this disorder is getting a good history, of course. Hip impingement pain is typically experienced anteriorly in the groin, but patients might also complain of associated lateral and posterior discomfort. Pain is often described as dull or aching in nature, worsening after prolonged periods of sitting. Occasionally, an exacerbation of sharp pain with activity is reported. Duration of symptoms is variable. Patients often report an inciting incident as the initial cause of the pain, but onset can also be insidious.
 AP pelvis demonstrates pistol-grip deformity (arrow).The physical examination is very important in these cases. Frequently, the patient has an antalgic gait. Range of motion is decreased and should be compared to the unaffected side. Typically, internal rotation with the hip at 90 degrees of flexion is markedly limited relative to the other side. Flexion and abduction can also be restricted compared to the opposite side.
AP pelvis demonstrates pistol-grip deformity (arrow).The physical examination is very important in these cases. Frequently, the patient has an antalgic gait. Range of motion is decreased and should be compared to the unaffected side. Typically, internal rotation with the hip at 90 degrees of flexion is markedly limited relative to the other side. Flexion and abduction can also be restricted compared to the opposite side.
The most important finding indicating hip impingement is a positive impingement test, which has been shown to be present in more than 90 percent of patients with confirmed FAI.1 The test is performed by having the patient supine on the examination table. The affected hip and knee are flexed to 90 degrees. The hip is then adducted and internally rotated in this flexed position. A positive test involves a sudden, often sharp pain in the hip. This maneuver often recreates the patient's symptoms. To complicate matters, there is a posterior impingement, which can be tested by forced external rotation of the hip while in full extension.
 Once the diagnosis of FAI is suspected, plain films should help to confirm the diagnosis, if one knows what to look for. There are a number of specialized imaging modalities that can be used to help determine the extent of the problem, as well as treatment options, but initially, a simple anteroposterior view of the pelvis and a lateral view of the affected hip should be adequate. The radiographic features of this disorder will vary depending on which type of impingement predominates (cam or pincer), but let's summarize the general findings.
Once the diagnosis of FAI is suspected, plain films should help to confirm the diagnosis, if one knows what to look for. There are a number of specialized imaging modalities that can be used to help determine the extent of the problem, as well as treatment options, but initially, a simple anteroposterior view of the pelvis and a lateral view of the affected hip should be adequate. The radiographic features of this disorder will vary depending on which type of impingement predominates (cam or pincer), but let's summarize the general findings.
Cam impingement demonstrates an aspherical femoral head with a predominate "bump," often referred to as a pistol-grip deformity. The cam impingement is more common in young males. These osseous bumps lead to a decreased femoral head-neck offset, which is defined by the distance between the widest diameter of the femoral head and the most prominent part of the femoral neck. It is thought that the main cause of cam impingement is growth abnormalities of the capital femoral epiphysis.
Pincer-type impingement demonstrates overcoverage of the acetabulum in relationship to the femoral head and a linear indentation at the head-neck junction of the femur. There are many ways of measuring the depth of the acetabulum. A software program has even been developed to determine the depth of the acetabulum.
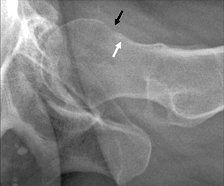 Lateral hip pincer-type impingement with linear erosion.My suggestion would be to compare the symptomatic hip to the asymptomatic hip. Compare the medial aspect of the acetabulum with the ilioishial line. There should be some visible gap between the two, and the ilioishial line should lie medial to the margin of the acetabulum. Then evaluate the amount of coverage of the femoral head. You can use the extrusion index, which is A + E divided by E. Normal should be about 25 percent. Again, compare the coverage of the femoral head with the asymptomatic side. The femoral head should never be completely covered by the acetabulum. About one-fourth of the head should lie outside the superior margin of the acetabulum.
Lateral hip pincer-type impingement with linear erosion.My suggestion would be to compare the symptomatic hip to the asymptomatic hip. Compare the medial aspect of the acetabulum with the ilioishial line. There should be some visible gap between the two, and the ilioishial line should lie medial to the margin of the acetabulum. Then evaluate the amount of coverage of the femoral head. You can use the extrusion index, which is A + E divided by E. Normal should be about 25 percent. Again, compare the coverage of the femoral head with the asymptomatic side. The femoral head should never be completely covered by the acetabulum. About one-fourth of the head should lie outside the superior margin of the acetabulum.
A pitfall to be aware of is that a pseudo-deep acetabulum can be produced on an anteroposterior radiograph that is centered over the hip.1 Do not use the AP spot view of the hip to determine the depth of the acetabulum. Only use the AP view of the pelvis due to differences in the central ray. The pincer-type impingement is more common in women. One can think of the pincer impingement as associated with acetabular pathomorphologies, but once the stage is set, most patients demonstrate a combination of both types of impingements, with one perhaps being more predominant.
 Left: Pitt�s pit (arrow) now indicative of impingement.Right: Os acetabuli (arrow) line of sclerosis (arrows), indicative of impingement.Secondary signs on radiographic findings are: herniation pits, ossification of the labrum and os acetabuli.2 In fact, I'm certain some of you will remember when "Pitt's pit" was once considered a normal finding, as was the os acetabuli. Now we must consider those findings indicative of impingement.
Left: Pitt�s pit (arrow) now indicative of impingement.Right: Os acetabuli (arrow) line of sclerosis (arrows), indicative of impingement.Secondary signs on radiographic findings are: herniation pits, ossification of the labrum and os acetabuli.2 In fact, I'm certain some of you will remember when "Pitt's pit" was once considered a normal finding, as was the os acetabuli. Now we must consider those findings indicative of impingement.
It is important to be aware that hip impingement syndrome frequently is present in spite of a reported normal radiographic study of the hip, either due to an inability to recognize the subtle changes or even the possibility of finding the problem before radiographic findings are present. The history and clinical findings are of utmost importance, including a positive impingement test. If the patient had previous films that were negative, I recommend requesting the films before relying on a radiology report. If films are not available, at least take the AP pelvis to determine if there are any radiographic findings that would indicate impingement. Early diagnosis is crucial for the patient to avoid the progression of impingement syndrome to osteoarthritis.
References
- Leunig M, Ganz R. Femoroacetabular impingement: a common cause of hip complaints leading to arthrosis [in German]. Unfallchirurg 2005;108:9-17.
- Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br 2005;87:1012-8.
- Ito K, Leunig M, Ganz R. Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Rel Res 2004;429:262-71.
- Tannast M, Siebenrock K, Anerson S, Femoroacetabular impingement: radiographic diagnosis - what the radiologist should know. AJR 2007;188:1540-52.
- Leunig M, Beck M, Kalhor M, et al. Juxta-articular cysts at the anterosuperior femoral neck: high prevalence in hips with femoro-acetabular impingement. Radiology2005;244:237-46.
Nenhum comentário:
Postar um comentário