SLAP Lesion/TEST
An Excellent Test for a SLAP Lesion
By Warren Hammer, MS, DC, DABCO
Has a patient ever complained of nonspecific posterior shoulder pain (usually in the overhead position)? There also may be a painful popping and a sense of looseness in the shoulder, and some positive impingement signs.1 If so, you could be dealing with a SLAP (superior labrum, anterior to posterior) lesion.The glenoid labrum is a fibrous rim that attaches to the periphery of the glenoid fossa and helps to deepen it, thereby increasing the surface area of the glenoid. This deepening helps stabilize the humeral head - especially in the midrange of glenohumeral motion, at which point the ligamentous capsular structures are lax.2The labrum also serves as an attachment for the glenohumeral ligaments.
A SLAP lesion originates at the superior posterior labrum to the biceps anchor and extends anteriorly on the superior labrum. The proximal biceps tendon originates from the supraglenoid tubercle of the glenoid and blends into the fibers of the labrum and capsule surrounding this insertion. With type 1 and type 3 SLAP lesions, the biceps attachment to the labrum is intact; with type 2 SLAP and other such lesions, the biceps are pulled away from the glenoid attachment. This lack of a firm attachment of the biceps to the glenoid results in glenohumeral instability. Therefore, a labral injury may occur without biceps involvement, especially when the injury is of the compression type, such as those that occur as the result of a fall or repetitive compression from overhead throwing.3
The common type 2 SLAP lesion, in which the biceps tendon is detached, is usually a traction-type injury by which the biceps causes an avulsion of the superior labrum (deceleration phase of throwing). The patient also may complain of biceps tendinopathy, popping and clicking, due to the torn labrum. The superior laxity created by the loss of the biceps insertion may lead to damage to the posterosuperior porton of the rotator cuff, which may be associated with chronic SLAP problems. Rotator cuff injuries are not usually found in acute SLAP lesions.3 It appears that shoulder instability may stress the biceps insertion, leading to biceps detachment, or biceps detachment may lead to shoulder instability. Since the biceps tendon helps resist anterior translation, and supports the inferior glenohumeral ligament when the shoulder is in abduction and external rotation (cocking phase of the throw), if the shoulder is already unstable, the biceps are forced to overwork by increasing its protective compressive force, causing increased stress to the superior labrum and biceps tendon complex.
It has been proven that abduction and external rotation of the shoulder during the cocking phase of throwing stresses the origin of the long head of the biceps tendon, and its attachment to the posterior labrum.4
Kim, et al.,5 created a test for SLAP lesions that was positive mostly for the type Z lesion. The biceps load test II had a sensitivity of 89.7 percent; a specificity of 96.9 percent; a positive-predictive value of 92.1 percent; a negative-predictive value of 95.5 percent; and a kappa coefficient of 0.815. The test is performed as follows: The supine patient's arm is elevated to 120¡ and externally rotated to its maximal point, with the elbow in the 90¡ flexed position and the forearm in the supinated position. The patient is asked to flex the elbow while being resisted by the examiner. This is the position that reproduces the mechanism in the development of type 2 SLAP lesions.
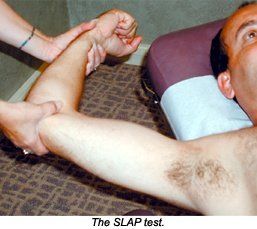
Forceful traction of the displaced biceps-superior labral complex occurs during the active contraction of the biceps muscle against resistance. Kim, et al., believe the test position changes the relative direction of the biceps fiber in a position of an oblique angle to the posterosuperior labrum, causing a peeling of the superior labrum off the glenoid margin.
The test is positive if the patient complains of pain during resisted elbow flexion, or if the patient complains of more pain from the test than the pain that was already present in the test position. The test is negative if pain is not elicited by resisted elbow flexion, or if the pre-existing pain is unchanged or diminished by resisted flexion.
References
- Kim S-H, Ha KK-I, Han K-Y. Biceps load test: a clinical test for superior labrum anterior and posterior lesions in shoulders with recurrent anterior dislocations. Amer J Sports Med1999; 27(3):300-307.
- Lippett FG. A modification of the gravity method of reducing anterior shoulder dislocations.Clin Orthop 1982; 165:259-260.
- Maffet MW, Lowe WR. Superior labral injuries. In: DeLee JC, Drez D. Orthopaedic Sports Medicine, Vol 1. Philadelphia: Saunders;2003.p.1046-1064.
- Rodosky MW, Harner CH, Fu FH. The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J sports Med1994;22:121-130.
- Kim S-H, et al. Biceps load test II: a clinical test for slap lesions of the shoulder. Arthroscopy: The Journal of Arthroscopic and Related Surgery 2001;17(2):160-164.
Warren Hammer, MS, DC, DABCO
Norwalk, Connecticut
Norwalk, Connecticut
Latest Test for Detecting SLAP Lesions
By Warren Hammer, MS, DC, DABCO
That painful clicking shoulder, especially in a thrower, could be a torn labrum usually referred to as a superior labral tear that is anterior to posterior in direction (SLAP) between the 10 and 2 o'clock position of the glenoid.
The labrum is located at the circumference of the glenoid cavity and is the attachment point of the shoulder capsule. Anchoring of the capsule to the glenoid labral rim is important for glenohumeral stability.1 Tearing of the labrum, which is attached to the glenoid, is an indicator that the capsule also is not attached at that location. There are four main types of SLAP lesions with the most common being the type 2, the only type where there is an actual detachment of both the labrum and biceps that inserts into the labrum.1
 Physical examination for a shoulder labral tear is equivocal and it's disheartening to realize that most of the labral tests are not very sensitive or specific. Tests such as O'Brien, the crank test, Speed test, anterior slide, the compression-rotation test, biceps load and Yergason test are no longer considered predictive for SLAP lesions,1,2 even when they reproduce a painful click. Kibler1 stated that no single test is diagnostic and recommended at least five tests before making a decision. When the O'Brien test was first presented, O'Brien reported that his test was 100 percent sensitive and 98.5 percent specific for labral tears. Guanche, et al.,3 used arthroscopic evaluation before surgery to determine if particular labral tests were as valid as they were supposed to be and found the O'Brien test to be 63 percent sensitive and 73 percent specific.
Physical examination for a shoulder labral tear is equivocal and it's disheartening to realize that most of the labral tests are not very sensitive or specific. Tests such as O'Brien, the crank test, Speed test, anterior slide, the compression-rotation test, biceps load and Yergason test are no longer considered predictive for SLAP lesions,1,2 even when they reproduce a painful click. Kibler1 stated that no single test is diagnostic and recommended at least five tests before making a decision. When the O'Brien test was first presented, O'Brien reported that his test was 100 percent sensitive and 98.5 percent specific for labral tears. Guanche, et al.,3 used arthroscopic evaluation before surgery to determine if particular labral tests were as valid as they were supposed to be and found the O'Brien test to be 63 percent sensitive and 73 percent specific.
He found similar results with other tests and concluded that a decision to proceed with surgery should not be based on clinical examination alone.3
Yang-Soo Kim, et al.,2 discovered a new test for superior labral tears of the shoulder. They used what they call the Passive Compression Test (PCT), which was performed independently by two physicians as the first test before any other diagnostic evaluation including MR arthrogram imaging was used. All the lesions were eventually verified by arthroscopic examination and arthroscopic surgeries. Of the 61 shoulders examined, 31 demonstrated a positive PCT and 30 demonstrated a negative test result. Of the 31 patients with a positive test, 27 had confirmed SLAP tears. Of the 30 patients with a negative PCT, 24 had intact superior labra whereas the other six had confirmed SLAP tears at surgery. The sensitivity of the test was 81.8 percent and the specificity was 85.7 percent. The positive predictive value (PPV) was 87.1 percent and the negative predictive value was 80 percent. "Sensitivity" of a test is defined as the probability that patients who truly should have the positive response have that response when the test is performed. When a test has a very high sensitivity, a negative clinical finding effectively rules out the diagnosis. "Specificity" of a test is defined as the probability that patients who should truly have a negative response, express a negative response when the test is performed. PPV is the probability that a patient who receives a positive test result will truly have a positive response (the actual pathology tested for).1 These percentages regarding the PCT are considered very good.
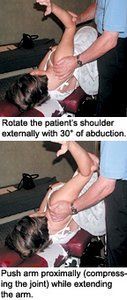
For the PCT, the patient lies sideways on the normal shoulder. The clinician stabilizes the shoulder at the acromioclavicular joint area with one hand and the patient's elbow with the other hand. Next, rotate the patient's shoulder externally with 30 degrees of abduction and then push the arm proximally (compressing the joint) while extending the arm. This should create a passive compression of the superior labrum onto the glenoid. All three motions should be performed at about the same time. The test is positive if it elicits pain or a painful click. The authors feel this test "reenacts the mechanisms of development of SLAP lesions." During external rotation and abduction of the humeral head, the long head of the biceps tendon is pulled laterally and will be under tensile tension as it wraps around the lesser tuberosity. This tension causes the superior labrum to shift from the superior glenoid rim. The second motion of extension of the shoulder with external rotation reproduces the late cocking phase of throwing. These motions have been found to increase the torsional stress at the origin of the long head of the biceps tendon and its attachment to the superior glenoid rim. The compressing of the humeral head "can aggravate the passive displacement of the unstable superior labrum on the glenoid."2 Many SLAP injuries occur due to a fall onto an outstretched arm, creating a compression force to the shoulder.
The authors state that a false-positive result may occur if there is anterior instability of the shoulder determined by the anterior apprehension test or anterior drawer test. So this test will be most accurate if anterior instability is first ruled out. Let us hope that this test remains valid for awhile.
References
- Hammer WI. Functional Soft-Tissue Examination and Treatment by Manual Methods, 3rded. Sudbury, Mass.: Jones & Bartlett, 2007:33-161.
- Yang-Soo Kim, Jung-Man Ha, Kee Yong, et al. The passive compression test: A new clinical test for superior labral tears of the shoulder. Am J Sports Med, 2007;35(9):1489-94.
- Guanche CA, Jones DC. Clinical testing for tears of the glenoid labrum. Arthroscopy,2003;19:517-23.
Nenhum comentário:
Postar um comentário